




What is Rheumatoid arthritis?
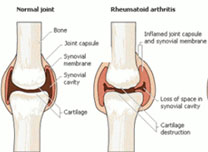
 Rheumatoid arthritis is usually called RA. RA is a chronic systemic inflammatory disease that causes pain, stiffness, and swelling in multiple
joints. RA is usually 3 times more common in women than men. RA causes joint lining to be inflamed and this leads to erosions of the cartilage
and bone and sometimes joint deformity. However, inflammation
sometimes can affect other organs as well such as eyes or lungs. Even though RA is a serious problem, the causes of RA are still unknown.
Rheumatoid arthritis is usually called RA. RA is a chronic systemic inflammatory disease that causes pain, stiffness, and swelling in multiple
joints. RA is usually 3 times more common in women than men. RA causes joint lining to be inflamed and this leads to erosions of the cartilage
and bone and sometimes joint deformity. However, inflammation
sometimes can affect other organs as well such as eyes or lungs. Even though RA is a serious problem, the causes of RA are still unknown.
What are symptoms?
 Most of people are not able to recognize that they are infected or not because RA usually occurs insidiously with a slow development of sings
and symptoms over weeks to months. However, some people sometimes recognize it early due to rapid onset. There are several symptoms that are
related with joint, which are pain, morning stiffness, warmth, deformity,
functional disability, baker’s cyst. There are also systemic symptoms such as fatigue, low grade fever, loss of appetite, and weight loss.
Most of people are not able to recognize that they are infected or not because RA usually occurs insidiously with a slow development of sings
and symptoms over weeks to months. However, some people sometimes recognize it early due to rapid onset. There are several symptoms that are
related with joint, which are pain, morning stiffness, warmth, deformity,
functional disability, baker’s cyst. There are also systemic symptoms such as fatigue, low grade fever, loss of appetite, and weight loss.
How would you know if you have Rheumatoid arthritis?
It is hard to figure out whether people are infected to RA or not because symptoms usually start late. In order to confirm it, people need to see a
doctor; however, there is no specific laboratory test yet. In order to check it, doctor should determine by observing at the symptoms and
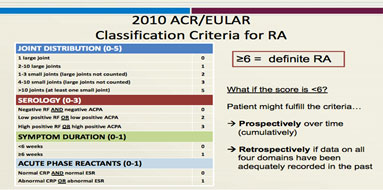
results from the physical exam, lab tests, and x-rays. There is also criteria classification for RA to confirm it.
Differences between Osteoarthritis and Rheumatoid arthritis
People are usually confused RA with OA; however, they are quite different. The peak age of onset is different. RA usually occurs between 35 and 50, but
OA usually occurs after 65. Obesity may cause OA, but it does not cause RA. The best difference to figure out between RA and OA is the duration of
stiffness. Both RA and OA have morning stiffness, but RA usually has more than 30 minutes, but OA usually stops before 30 minutes.
Medications
There are four different categories for Rheumatoid arthritis: adjunctive therapy, non-biologic DMARDs, TNF-a inhibitors, and non-TNF biologics.
- Hydroxychloroquine (HCQ Plaquenil)
- Sulfasalazine (Azulfidine)
- Minocycline (Minocin)
- Tofacitinib (Xeljanz)
- Etanercept (Enbrel)
- Inflixamab (Remicade)
- Adalmumab (Humira)
- Golimumab (simponi)
- Certolizumab (Cimzia)
- Abatacept (Orencia)
- Rituximab (Rituxan)
- Tocilizumab (Actemra)
- Anakinra (kineret)
Additional links:
http://www.cdc.gov/arthritis/index.htm
http://www.cdc.gov/arthritis/basics/rheumatoid.htm
http://www.arthritis.org/about-arthritis/types/rheumatoid-arthritis/treatment.php
References:
http://www.cdc.gov/arthritis/basics/rheumatoid.html
http://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Rheumatoid-Arthritis
http://www.cdc.gov/arthritis/temp/pilots-201208/pilot1/online/arthritis-challenge/01-ArthritisBasics/rheumtd.htm
http://www.arthritis.org/about-arthritis/types/rheumatoid-arthritis/treatment.php
http://www.eular.org/myUploadData/files/RA%20Class%20Slides%20ACR_Web.pdf
